Your shoulder connects three bones together: it connects the humerus (upper arm bone) to the clavicle 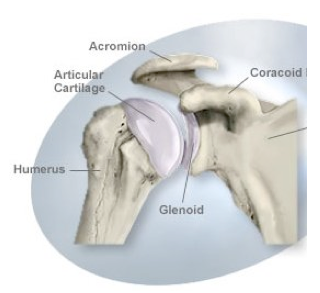 (collarbone) and the scapula (shoulder blade). It is arranged in what is known as a “ball and socket” joint configuration, where the humeral head rotates within the glenoid fossa.
(collarbone) and the scapula (shoulder blade). It is arranged in what is known as a “ball and socket” joint configuration, where the humeral head rotates within the glenoid fossa.
The shoulder is stabilized by four rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis) that keep the humeral head in place. Your shoulder also serves as an important attachment for numerous muscles that allow the shoulder and arm to move, such as the deltoids, rhomboids, trapezius, among others.
What is instability of the shoulder?
You may have what is known as shoulder instability if your shoulder moves out of place. This is caused by the humeral head slipping out of the socket of the glenoid fossa. Shoulder instability manifests as excessive laxity of the shoulder joint in one or more directions. Instability is considered, as opposed to laxity, when there is loss of function or when there is difficulty doing normal daily activities.
How does shoulder instability manifest?
People who suffer from shoulder instability typically complain of pain in the shoulder, or the feeling of 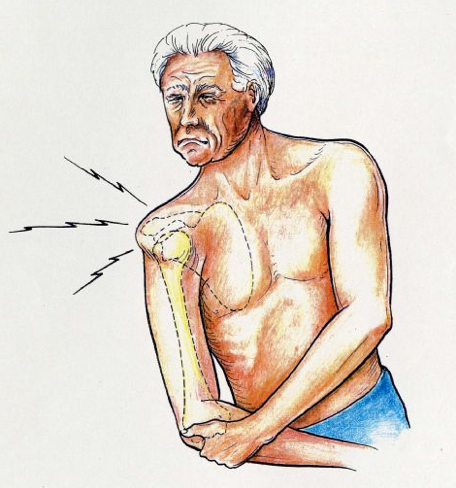 “looseness” of the shoulder. You may also experience “popping” or “clicking” in your shoulder with particular movements. Some patients complain of numbness or weakness. Symptoms such as these occur during normal activities, especially those with overhead movements. They can occur during swimming, weight training, sports activities, among others. You may also notice that the symptoms get worse over time. Not all patients will have a history of a precipitating event that triggered the symptos.
“looseness” of the shoulder. You may also experience “popping” or “clicking” in your shoulder with particular movements. Some patients complain of numbness or weakness. Symptoms such as these occur during normal activities, especially those with overhead movements. They can occur during swimming, weight training, sports activities, among others. You may also notice that the symptoms get worse over time. Not all patients will have a history of a precipitating event that triggered the symptos.
How is shoulder instability treated?
The treatment for symptomatic shoulder injury can be conservative or surgical. The nonsurgical option should always be considered first before surgery. There are risks inherent in surgery, and it should be reserved for the more severe cases.
An acute dislocation of the arm from the shoulder socket should be immediately treated by reducing (putting back in place) the joint. Ideally this should be done by a trained professional to reduce the likelihood of damage to the shoulder. The shoulder should be then immobilized with a sling, and cold compress applied every two to three hours to reduce swelling and inflammation. The patient should then be brought to a physician for a complete history and physical examination. Immobilization for dislocated joints may require 3 to 8 weeks for healing.
The goal of nonoperative therapy is to improve the stability of the joint by strengthening the muscles of the shoulder. This is accomplished through a progressive program of physical therapy and rehabilitation. Physical therapy utilizes a program of neuromuscular training, strengthening the compressor muscles, and improving shoulder stability. Rehabilitation of the joint focuses on retraining the shoulder to perform movements at a more stable range.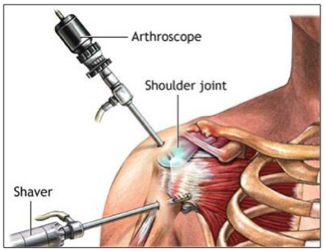
When would surgery be needed?
Surgery is an option that is reserved for patients with severe instability, i.e., those who have their activities of daily living adversely affected. Candidates for surgery should have attempted conservative treatment prior to the operation. The goal of surgery is to stabilize the shoulder joint by tightening the shoulder attachments, providing reattachments or to replace torn tissues.




{kind=link}
{kind=link}
{kind=link}
{kind=link}